Rapid, accurate, clinical decision support
Advanced digital signal processing of brain electrical activity data at the core of FDA cleared AI, machine learning derived algorithms, empower clinicians to rule out likelihood of intracranial hemorrhage & objectively assess for concussion

How BrainScope Works : Use of EEG based brain biomarkers to assess head injured patients and assist clinicians in their diagnosis
Exceptionally well validated
12 years of development funded in part by 8 Department of Defense studies and 2 GE/NFL Head Challenge grants
Sensitivity well above that of commonly used diagnostic tools for other medical conditions

BrainScope Structural Injury Classifier (SIC) was demonstrated to objectively identify the likelihood of an intracranial hemorrhage with 99% sensitivity to even the smallest amount of detectable blood (≥1 mL).
Here's what makes it work
Hardware
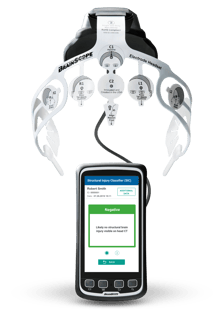
The handheld medical device acquires brain electrical activity data recorded from the proprietary 8-electrode disposable headset
AI Derived Biomarker Algorithms
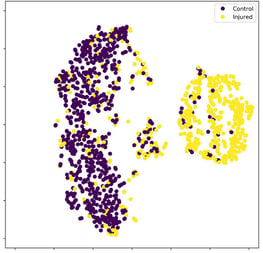
With brain electrical activity features as core inputs to machine learning classifier building methods, distinctive profiles of TBI are identified
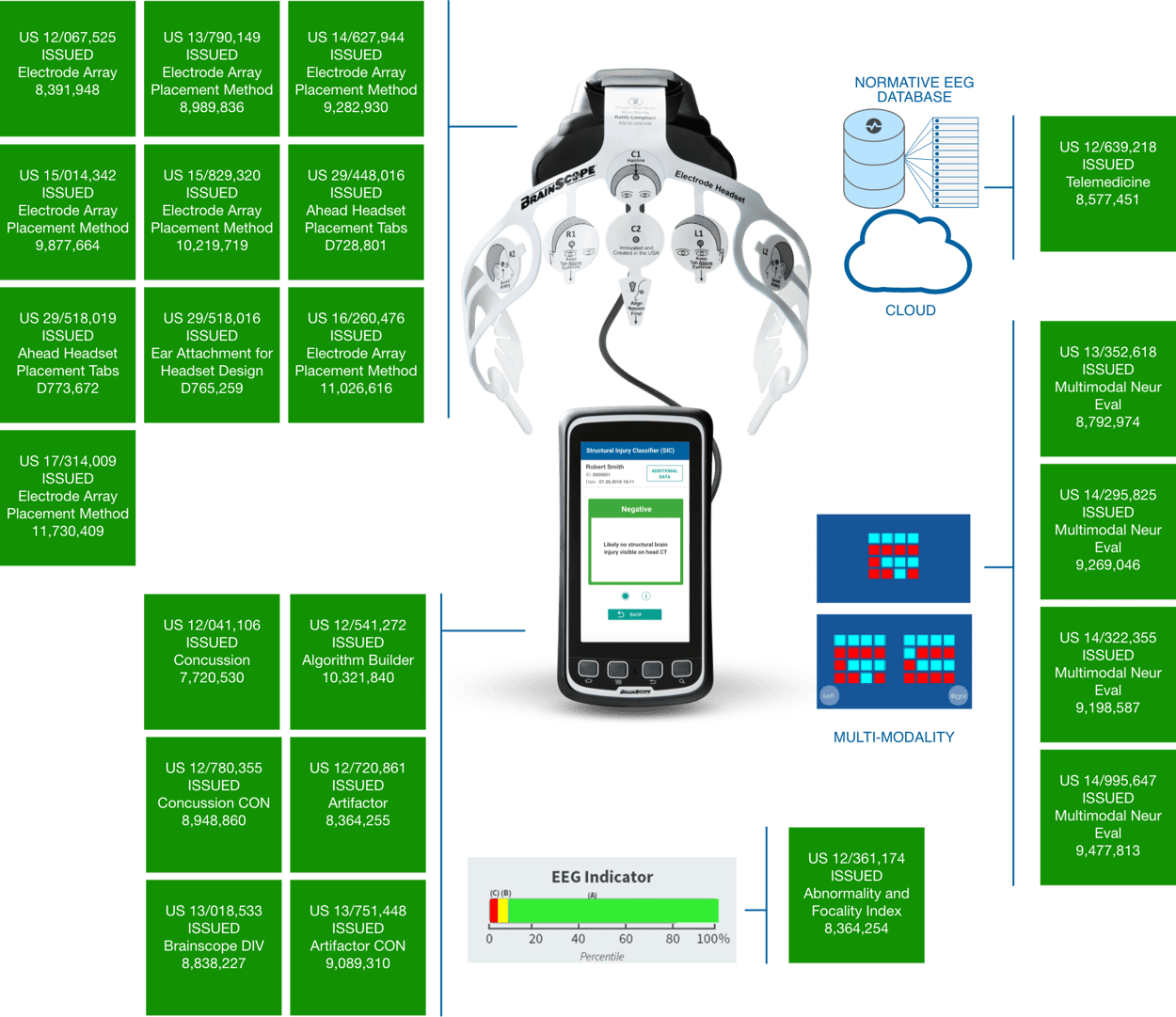


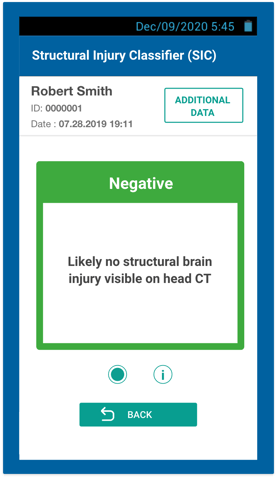
Structural Injury Classifier (SIC)
A multimodal AI derived algorithm that indicates the likelihood of being negative for brain bleed on a CT scan and identifies the need for further evaluation
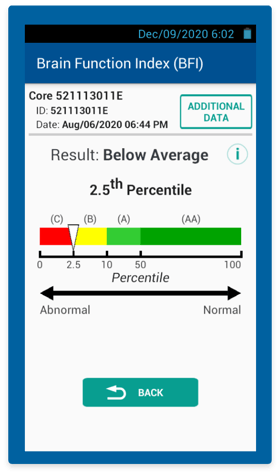
Brain Function Index (BFI) textpadding
A brain electrical activity based algorithm for the assessment of brain function impairment, obtained from the same recording used to compute the SIC—can aid in early clinical diagnosis of concussion and referrals
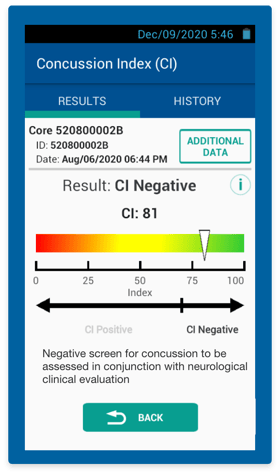
Concussion Index (CI)
An objective multimodal AI derived algorithm with brain electrical activity at its core—aids in clinical diagnosis of concussion
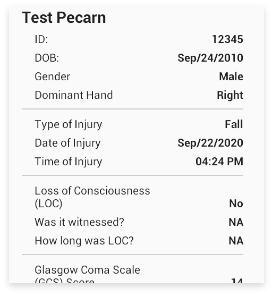
Digitized & Neurocognitive Clinical Assessments
Includes assessments commonly used by clinicians to assess head injured patients, including PECARN Decision Rule for pediatrics

Our research team
Led by our Chief Scientific Officer, Leslie S. Prichep, PhD, our vibrant research group has experience beyond traumatic brain injury into neurological conditions such as stroke, Alzheimer's disease, depression, and cognitive decline.
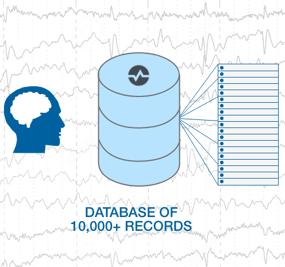
The BrainScope algorithms were developed by applying advanced AI/machine learning technology to extensive patient data, including EEG data, symptoms, CT scan and neurological test results. As the database grows, machine learning capabilities can identify additional data patterns, enhancing future technology, advancing the potential clinical application of head injury assessment, and identifying new indications for use, using the neurotechnology platform that has been developed by BrainScope over the past decade.
Dr. Prichep and her team continue to work on furthering our understanding of brain health.
Our research partners

University of Rochester Medical Center

Johns Hopkins Medicine

Texas Tech University
